Cure For Bursitis In Ball Of Foot
Overview
There are about 160 bursae in the human body. These little, fluid-filled sacs cushion pressure and lubricate points between our bones, tendons, and muscles near our joints. The bursae are lined with synovial cells. Synovial cells produce a lubricant that reduces friction. This cushioning and lubrication allows our joints to move easily. When a person has bursitis, inflammation of the bursa, movement or pressure is painful. Overuse, injury and sometimes an infection from gout or rheumatoid arthritis may cause bursitis.
Causes
The calcaneal bursa can become inflamed in patients with heel spurs or in patients with poor-fitting shoes (eg, high heels). Inflammation can occur secondarily from Achilles tendinitis, especially in young athletes. Patients exhibit tenderness to palpation of the bursa anterior to the Achilles tendon on both the medial and lateral aspects. They have pain with movement, which is worsened with dorsiflexion.
Symptoms
Common signs and symptoms associated with infracalcaneal bursitis include redness under the heel. Pain and swelling under the heel. Pain or ache in the middle part of the underside of the heel. Heel pain or discomfort that increases with prolonged weight-bearing activities.
Diagnosis
When you are experiencing Achilles pain at the back of your heel, a visit to the doctor is always recommended. Getting a proper diagnosis is important so you can treat your condition correctly. A doctor visit is always recommended.
Non Surgical Treatment
Relieving the symptoms of bursitis initially focuses on taking the pressure off the bursa. This can be done with proper cushioning, inserts, or footwear but may require surgery if it is a bone formation problem (i.e. Huglund's Deformity). If your bursitis is caused by an infection (septic bursitis), the doctor will probably drain the bursa sac with a needle and prescribe antibiotics to treat the infection.
Surgical Treatment
Surgery is rarely done strictly for treatment of a bursitis. If any underlying cause is the reason, this may be addressed surgically. During surgery for other conditions, a bursa may be seen and removed surgically.
There are about 160 bursae in the human body. These little, fluid-filled sacs cushion pressure and lubricate points between our bones, tendons, and muscles near our joints. The bursae are lined with synovial cells. Synovial cells produce a lubricant that reduces friction. This cushioning and lubrication allows our joints to move easily. When a person has bursitis, inflammation of the bursa, movement or pressure is painful. Overuse, injury and sometimes an infection from gout or rheumatoid arthritis may cause bursitis.
Causes
The calcaneal bursa can become inflamed in patients with heel spurs or in patients with poor-fitting shoes (eg, high heels). Inflammation can occur secondarily from Achilles tendinitis, especially in young athletes. Patients exhibit tenderness to palpation of the bursa anterior to the Achilles tendon on both the medial and lateral aspects. They have pain with movement, which is worsened with dorsiflexion.
Symptoms
Common signs and symptoms associated with infracalcaneal bursitis include redness under the heel. Pain and swelling under the heel. Pain or ache in the middle part of the underside of the heel. Heel pain or discomfort that increases with prolonged weight-bearing activities.
Diagnosis
When you are experiencing Achilles pain at the back of your heel, a visit to the doctor is always recommended. Getting a proper diagnosis is important so you can treat your condition correctly. A doctor visit is always recommended.
Non Surgical Treatment
Relieving the symptoms of bursitis initially focuses on taking the pressure off the bursa. This can be done with proper cushioning, inserts, or footwear but may require surgery if it is a bone formation problem (i.e. Huglund's Deformity). If your bursitis is caused by an infection (septic bursitis), the doctor will probably drain the bursa sac with a needle and prescribe antibiotics to treat the infection.
Surgical Treatment
Surgery is rarely done strictly for treatment of a bursitis. If any underlying cause is the reason, this may be addressed surgically. During surgery for other conditions, a bursa may be seen and removed surgically.
How To Relieve Hammer Toe Pain
 Overview
Overview
Hammer, mallet, and claw toes have distinctive differences that can assist you in determining what kind of toe problem you are dealing with. All three conditions deal with toes that are curved into abnormal positions, which possibly look strange and may cause pain. Typically, the big toe is not affected by these problems. A Hammer toes tends to bend downward at the center of a toe joint. It generally affects your second toe. The affliction causes the center of your toe to rise and is often accompanied with a bony lump.
Causes
While most cases of hammertoes are caused by an underlying muscle imbalance, it may develop as a result of several different causes, including arthritis, a hereditary condition, an injury, or ill-fitting shoes. In some cases, patients develop hammertoes after wearing shoes or stockings that are too tight for long periods of time. These patients usually develop hammertoes in both feet.
 Symptoms
Symptoms
Hammertoe and mallet toe feature an abnormal bend in the joints of one or more of your toes. Moving the affected toe may be difficult or painful. Corns and calluses can result from the toe rubbing against the inside of your shoes. See your doctor if you have persistent foot pain that affects your ability to walk properly.
Diagnosis
Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe. If the deformed toe is very painful, your doctor may recommend that you have a fluid sample withdrawn from the joint with a needle so the fluid can be checked for signs of infection or gout (arthritis from crystal deposits).
Non Surgical Treatment
Many people start by treating the problem themselves when they have a painful corn or callus. They try to remove the corn by cutting it off or by applying strong acids, and they try to cushion the toe by applying cushioned pads. Because these treatments can Hammer toe be difficult to perform by oneself (and should never be done by oneself when the patient is diabetic or circulation is poor), and because these treatments only treat the symptom, not the structural deformity that causes their symptom, these treatments can often provide only limited success, and often any success is for only short periods of time. Changes in shoe choices and various types of paddings and other appliances may help, too. For longer-lasting help, we must examine the cause of the deformity. The reason for knowing the cause is that the type of treatment will vary, depending upon the cause of the complaint. Orthotics help control the causes of certain types of contracted toes, (those caused by flexor stabilization, for example), but not other types.
Surgical Treatment
Curative treatment of hammertoes varies depending upon the severity of the deformity. When the hammertoe is flexible, a simple tendon release in the toe works well. The recovery is rapid often requiring nothing more that a single stitch and a Band-Aid. Of course if several toes are done at the same time, the recovery make take a bit longer.
Hallux Valgus Correction
Overview
 A bunion (a.k.a Hallux Valgus) is a common foot condition associated with a prominent bump on the inside of the forefoot (see Figure 1). The word bunion? comes from the Greek root for the word turnip. Bunions can lead to discomfort over the prominence, especially if patients wear tight fitting shoes. It is common for bunions to run in family? and gradually increase over time. The vast majority of bunions can be managed successfully with basic non-operative treatment. Surgery is reserved for patients who have persistent symptoms in spite of appropriate non-operative treatment.
A bunion (a.k.a Hallux Valgus) is a common foot condition associated with a prominent bump on the inside of the forefoot (see Figure 1). The word bunion? comes from the Greek root for the word turnip. Bunions can lead to discomfort over the prominence, especially if patients wear tight fitting shoes. It is common for bunions to run in family? and gradually increase over time. The vast majority of bunions can be managed successfully with basic non-operative treatment. Surgery is reserved for patients who have persistent symptoms in spite of appropriate non-operative treatment.
Causes
Despite the popular belief, wearing high heels and too-narrow shoes does not cause bunions. Wearing them can irritate, aggravate, or accelerate the formation of the bunion, but are not the root cause. Bunions are more commonly inherited, if your parents or grandparents had bunions, you may also get one. Bunions can also be caused by trauma or injury to the joints, ligaments, or bones of the foot.
Symptoms
The symptoms of a bunion include the following development of a firm bump on the outside edge of the foot, at the base of the big toe, redness, swelling, or pain at or near the MTP joint, corns or other irritations caused by the overlap of the first and second toes, restricted or painful motion of the big toe.
Diagnosis
Physical examination typically reveals a prominence on the inside (medial) aspect of the forefoot. This represents the bony prominence associated with the great toe joint ( the medial aspect of the first metatarsal head). The great toe is deviated to the outside (laterally) and often rotated slightly. This produces uncovering of the joint at the base of the big toe (first metatarsophalangeal joint subluxation). In mild and moderate bunions, this joint may be repositioned back to a neutral position (reduced) on physical examination. With increased deformity or arthritic changes in the first MTP joint, this joint cannot be fully reduced. Patients may also have a callus at the base of their second toe under their second metatarsal head in the sole of the forefoot. Bunions are often associated with a long second toe.
Non Surgical Treatment
Getting rid of a Bunion is almost impossible without surgery. Foot and toe exercises can help. Foam pads can reduce the pressure on the joint. Ice packs and anti-inflammatory medication can help reduce swelling. The progress of a Bunion can be slowed or even halted, especially if it is caused by ill-fitting footwear. Of course the best course of action is to not wear pointy-toed high-heel shoes to begin with. But if you have worn improper footwear and now want to stop the progress of Bunions. 
Surgical Treatment
Bunion surgery is occasionally required when the bunion deformity is too advanced for conservative treatment to work. Your surgeon will usually cut an angular section from the bone to correct the alignment. In some cases, multiple toes may need to be straighten.
Over-Pronation
Overview
Everyone pronates! Contrary to popular misconception it is healthy and normal. The problem begins when one or both of our feet pronate too much. When the arches flex too far inward or stay collapsed for too long pronation is considered excessive. We call this overpronation. Overpronation is by far the most common foot type. Pronation is not linked one-to-one with low arches. Although pronation lowers the arches, this does not mean that only those with low arches overpronate. People with high arches can also overpronate! Some of us have always overpronated, for others overpronation develops with age, weight gain, regular standing work or intensive exercise.
Causes
Although there are many factors that can contribute to the development of these conditions, improper biomechanics of the body plays a large and detrimental role in the process. Of the many biomechanical elements involved, foot and ankle function perhaps contribute the most to these aches and pains.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
When sitting, an over-pronating foot appears quite normal, i.e. showing a normal arch with room under the underside of the foot. The moment you get up and put weight on your feet the situation changes: the arches lower and the ankle slightly turns inwards. When you walk or run more weight is placed on the feet compared to standing and over-pronation will become more evident. When walking barefoot on tiles or timber floors over-pronation is more visible, compared to walking on carpet or grass.
Non Surgical Treatment
Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. This orthotics should be designed with appropriate arch support and medial rear foot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improperly fitting footwear can lead to additional foot problems. If the problem persists, consult your foot doctor.
Surgical Treatment
HyProCure implant. A stent is placed into a naturally occurring space between the ankle bone and the heel bone/midfoot bone. The stent realigns the surfaces of the bones, allowing normal joint function. Generally tolerated in both pediatric and adult patients, with or without adjunct soft tissue procedures. Reported removal rates, published in scientific journals vary from 1%-6%.
Everyone pronates! Contrary to popular misconception it is healthy and normal. The problem begins when one or both of our feet pronate too much. When the arches flex too far inward or stay collapsed for too long pronation is considered excessive. We call this overpronation. Overpronation is by far the most common foot type. Pronation is not linked one-to-one with low arches. Although pronation lowers the arches, this does not mean that only those with low arches overpronate. People with high arches can also overpronate! Some of us have always overpronated, for others overpronation develops with age, weight gain, regular standing work or intensive exercise.
Causes
Although there are many factors that can contribute to the development of these conditions, improper biomechanics of the body plays a large and detrimental role in the process. Of the many biomechanical elements involved, foot and ankle function perhaps contribute the most to these aches and pains.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
When sitting, an over-pronating foot appears quite normal, i.e. showing a normal arch with room under the underside of the foot. The moment you get up and put weight on your feet the situation changes: the arches lower and the ankle slightly turns inwards. When you walk or run more weight is placed on the feet compared to standing and over-pronation will become more evident. When walking barefoot on tiles or timber floors over-pronation is more visible, compared to walking on carpet or grass.
Non Surgical Treatment
Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. This orthotics should be designed with appropriate arch support and medial rear foot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improperly fitting footwear can lead to additional foot problems. If the problem persists, consult your foot doctor.
Surgical Treatment
HyProCure implant. A stent is placed into a naturally occurring space between the ankle bone and the heel bone/midfoot bone. The stent realigns the surfaces of the bones, allowing normal joint function. Generally tolerated in both pediatric and adult patients, with or without adjunct soft tissue procedures. Reported removal rates, published in scientific journals vary from 1%-6%.
Treating Calcaneal Apophysitis
Overview
Sever?s disease is repetitive micro trauma or overuse of the heel in young athletes. Sever?s is caused by overloading the insertion of the Achilles tendon onto the calcaneus and the apophyseal growth plate. Active Children (7 to 15 years), particularly during the pubertal growth spurt or at the beginning of a sport season (e.g. gymnasts, basketball and football players), often suffer from this condition.
Causes
There are usually two root causes of Sever?s disease that we?ve found that effect young athletes. Arches are not supported causing a dysfunctional run, jump, and landing. The calves (gastrocnemius and soleus muscles) are overworked, tight, and do not allow proper movement of foot which puts extreme pressure on the Achilles? tendon, in turn irritating the growth plate in the heel.
Symptoms
Pain is reproduced through a gentle squeeze of the back of the heel. Children may present with a limp or ?Bouncy gait?. Pain is worse barefoot and often present in the mornings and post exercise. The pain is located at the back of the heel, with localized swelling of the area.
Diagnosis
The x-ray appearance usually shows the apophysis to be divided into multiple parts. Sometimes a series of small fragments is noted. Asymptomatic heels may also show x-ray findings of resporption, fragmentation and increased density. But they occur much less often in the normal foot. Pulling or ?traction? of the Achilles tendon on the unossified growth plate is a likely contributing factor to Sever?s disease. Excessive pronation and a tight Achilles and limited dorsiflexion may also contribute to the development of this condition.
Non Surgical Treatment
Treatment includes modifying activities and resting to reduce pain and inflammation and take pressure off the growth center. Ice can also be very helpful in relieving symptoms, as well as anti-inflammatory medication. A physical therapy program should be initiated to stretch tight calf muscles and strengthen the ankle muscles to relieve tension on the growth center. Shoes with padded heel surfaces and good arch support can decrease pain. Cleats may need to be avoided for some time to help reduce symptoms. The doctor may also recommend gel heel cups or supportive shoe inserts.
Recovery
Receiving the initial diagnosis of Sever?s disease can be scary, and while the situation is painful, there is good news. If treated properly and quickly, Sever?s disease is temporary and will have no long-term effects on the athlete.
Sever?s disease is repetitive micro trauma or overuse of the heel in young athletes. Sever?s is caused by overloading the insertion of the Achilles tendon onto the calcaneus and the apophyseal growth plate. Active Children (7 to 15 years), particularly during the pubertal growth spurt or at the beginning of a sport season (e.g. gymnasts, basketball and football players), often suffer from this condition.
Causes
There are usually two root causes of Sever?s disease that we?ve found that effect young athletes. Arches are not supported causing a dysfunctional run, jump, and landing. The calves (gastrocnemius and soleus muscles) are overworked, tight, and do not allow proper movement of foot which puts extreme pressure on the Achilles? tendon, in turn irritating the growth plate in the heel.
Symptoms
Pain is reproduced through a gentle squeeze of the back of the heel. Children may present with a limp or ?Bouncy gait?. Pain is worse barefoot and often present in the mornings and post exercise. The pain is located at the back of the heel, with localized swelling of the area.
Diagnosis
The x-ray appearance usually shows the apophysis to be divided into multiple parts. Sometimes a series of small fragments is noted. Asymptomatic heels may also show x-ray findings of resporption, fragmentation and increased density. But they occur much less often in the normal foot. Pulling or ?traction? of the Achilles tendon on the unossified growth plate is a likely contributing factor to Sever?s disease. Excessive pronation and a tight Achilles and limited dorsiflexion may also contribute to the development of this condition.
Non Surgical Treatment
Treatment includes modifying activities and resting to reduce pain and inflammation and take pressure off the growth center. Ice can also be very helpful in relieving symptoms, as well as anti-inflammatory medication. A physical therapy program should be initiated to stretch tight calf muscles and strengthen the ankle muscles to relieve tension on the growth center. Shoes with padded heel surfaces and good arch support can decrease pain. Cleats may need to be avoided for some time to help reduce symptoms. The doctor may also recommend gel heel cups or supportive shoe inserts.
Recovery
Receiving the initial diagnosis of Sever?s disease can be scary, and while the situation is painful, there is good news. If treated properly and quickly, Sever?s disease is temporary and will have no long-term effects on the athlete.
Achilles Tendon Rupture Thompson Testing
Overview
 An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears.
An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears.
Causes
The tendon usually ruptures without any warning. It is most common in men between the ages of 40-50, who play sports intermittently, such as badminton and squash. There was probably some degeneration in the tendon before the rupture which may or may not have been causing symptoms.
Symptoms
It is important to know that pain at the back of the heel is not always due to Achilles tendon rupture. It may be due to bursitis (fluid accumulation in the heel due to repeated irritation) and tendonitis (pain along the Achilles tendon due to constant friction and irritation). The above disorders tend to improve with use of pain medications and rest, whereas Achilles tendon rupture requires surgery and/or a cast.
Diagnosis
Other less serious causes of pain in the back of the lower leg include Achilles tendonitis or bursitis. To distinguish between these possibilities, your physician will take a thorough history and examine your lower leg to look for signs of a rupture. The presence of a defect in the tendon that can be felt, evidence of weakness with plantarflexion, and a history consistent with Achilles tendon rupture are usually sufficient for diagnosis. Your physician may also perform a ?Thompson test,? which consists of squeezing the calf muscles of the affected leg. With an intact Achilles tendon, the foot will bend downward; however, with a complete rupture of the tendon, the foot will not move. In cases where the diagnosis is equivocal, your physician may order an MRI of the leg to diagnose a rupture of the Achilles tendon.
Non Surgical Treatment
There is no definitive protocol for conservative management. Traditionally, conservative treatment involved immobilisation in a cast or boot, with initial non-weight bearing. Recently, good results have been achieved with functional bracing and early mobilisation, and it is common to be immediately weight-bearing in an orthotic. Conservative management reduces the chance of complications, such as infection. There is a risk the tendon can heal too long and more slowly. 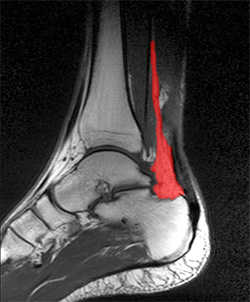
Surgical Treatment
There are a variety of ways to repair an Achilles tendon rupture. The most common method is an open repair. This starts with an incision made on the back of the lower leg starting just above the heel bone. After the surgeon finds the two ends of the ruptured tendon, these ends are sewn together with sutures. The incision is then closed. Another repair method makes a small incision on the back of the lower leg at the site of the rupture. A series of needles with sutures attached is passed through the skin and Achilles tendon and then brought out through the small incision. The sutures are then tied together. The best surgical technique for your Achilles rupture will be determined by your orthopaedic foot and ankle surgeon.
Prevention
To reduce your chance of developing Achilles tendon problems, follow the following tips. Stretch and strengthen calf muscles. Stretch your calf to the point at which you feel a noticeable pull but not pain. Don't bounce during a stretch. Calf-strengthening exercises can also help the muscle and tendon absorb more force and prevent injury. Vary your exercises. Alternate high-impact sports, such as running, with low-impact sports, such as walking, biking or swimming. Avoid activities that place excessive stress on your Achilles tendons, such as hill running and jumping activities. Choose running surfaces carefully. Avoid or limit running on hard or slippery surfaces. Dress properly for cold-weather training and wear well-fitting athletic shoes with proper cushioning in the heels. Increase training intensity slowly. Achilles tendon injuries commonly occur after abruptly increasing training intensity. Increase the distance, duration and frequency of your training by no more than 10 percent each week.
Leg Length Discrepancy Surgery
Overview
There are many different conditions in childhood and adult life that can lead to deformity of a limb or difference in leg lengths. Treatment for these conditions depends on the condition being treated, the age of the child and the amount of deformity or shortening. Generally, only a final difference of leg length of 2cm or more requires surgical treatment. An outline of treatment options is given below.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
Back pain along with pain in the foot, knee, leg and hip on one side of the body are the main complaints. There may also be limping or head bop down on the short side or uneven arm swinging. The knee bend, hip or shoulder may be down on one side, and there may be uneven wear to the soles of shoes (usually more on the longer side).
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
Whether or not treatment should be pursued depends on the amount of discrepancy. In general, no treatment (other than a heel life, if desired) should be considered for discrepancies under two centimeters. If the discrepancy measures between two and five centimeters, one might consider a procedure to equalize leg length. Usually, this would involve closure of the growth plate on the long side, thereby allowing the short side to catch up; shortening the long leg; or possibly lengthening the short leg.

Surgical Treatment
The bone is lengthened by surgically applying an external fixation device to the leg. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins, or both. A small crack is made in the bone and the frame creates tension when the patient or family member turns its dial. This is done several times each day. The lengthening process begins approximately five to 10 days after surgery. The bone may lengthen 1 millimeter per day, or approximately 1 inch per month. Lengthening may be slower in a bone that was previously injured. It may also be slower if the leg was operated on before. Bones in patients with potential blood vessel abnormalities, such as cigarette smokers, may also need to be lengthened more slowly. The external fixator is worn until the bone is strong enough to support the patient safely. This usually takes about three months for each inch. Factors such as age, health, smoking and participation in rehabilitation can affect the amount of time needed.
There are many different conditions in childhood and adult life that can lead to deformity of a limb or difference in leg lengths. Treatment for these conditions depends on the condition being treated, the age of the child and the amount of deformity or shortening. Generally, only a final difference of leg length of 2cm or more requires surgical treatment. An outline of treatment options is given below.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
Back pain along with pain in the foot, knee, leg and hip on one side of the body are the main complaints. There may also be limping or head bop down on the short side or uneven arm swinging. The knee bend, hip or shoulder may be down on one side, and there may be uneven wear to the soles of shoes (usually more on the longer side).
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
Whether or not treatment should be pursued depends on the amount of discrepancy. In general, no treatment (other than a heel life, if desired) should be considered for discrepancies under two centimeters. If the discrepancy measures between two and five centimeters, one might consider a procedure to equalize leg length. Usually, this would involve closure of the growth plate on the long side, thereby allowing the short side to catch up; shortening the long leg; or possibly lengthening the short leg.
Surgical Treatment
The bone is lengthened by surgically applying an external fixation device to the leg. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins, or both. A small crack is made in the bone and the frame creates tension when the patient or family member turns its dial. This is done several times each day. The lengthening process begins approximately five to 10 days after surgery. The bone may lengthen 1 millimeter per day, or approximately 1 inch per month. Lengthening may be slower in a bone that was previously injured. It may also be slower if the leg was operated on before. Bones in patients with potential blood vessel abnormalities, such as cigarette smokers, may also need to be lengthened more slowly. The external fixator is worn until the bone is strong enough to support the patient safely. This usually takes about three months for each inch. Factors such as age, health, smoking and participation in rehabilitation can affect the amount of time needed.